
This is a monthly update on my glycemic management of type 1 diabetes (T1DM) using Humalog and Lantus insulin injections with resistance exercise and a ketogenic whole-food diet as described in my book, The Ketogenic Diet for Type 1 Diabetes also available on Amazon in print.
I had stopped doing snatch and clean and jerk exercises in October to allow my left rotator cuff to heal. I originally injured it in March 2017 and it was primarily bothersome holding the bar overhead sometimes, but not others. I did notice it at other times, particularly when sleeping, but seemed pretty minor overall. I initially thought it would just go away, but after six months of it continuing to nag me, I sought a restorative plan to heal it. As mentioned I stopped all overhead movements, but in addition I found a book: Shoulder Pain? The Solution & Prevention: Fourth Edition, by John M. Kirsch M.D. In the book he states that most shoulder problems are due to contraction of the CA arch which results in shoulder impingement which in turn results in injury to the underlying rotator cuff. The rotator cuff is responsible for external rotation of the shoulder. External rotation is used in a minority of sports, but it is used extensively in olympic weightlifting. A more common example of external shoulder rotation is a backhand tennis swing. Dr. Kirsch explains “The CA arch is a curved structure in the shoulder that overlies the rotator cuff tendons and includes the coracoacromial ligament, the acromion, the coracoid process and other ligament’s connecting the acromion and the coracoid process.” The solution is passive hanging from a pull-up bar to lengthen the CA arch and light-weight dumbbell exercises to strengthen the rotator cuff muscles which I started a month ago. I am just now noticing that I am no longer experiencing any discomfort in my shoulder so I am going to start back with light weight snatch overhead squats first before returning to the actual olympic lifts. In October, I continued once daily weightlifting workouts and added just added the snatch overhead squats alternating with farmers carry to the two other exercises per day (squat and deadlift) all lasting about 2 hours including warmup, rest between lifts, and cool down.
Glycemic Management Results for October 2017
My October glycemic results were similar to previous time periods with more hypoglycemia and hyperglycemia than I would like and I only spent 50% of time with a blood glucose (BG) between 61 and 110 mg/dl (my goal is 70%). My insulin doses varyed up and down in response to low or high BG in the range of 30 to 40 IU/day or so with no definite up or down trends. Fortunately, I had no symptoms of hypoglycemia in October.
Below are my mean BG values, mean insulin doses, and BG frequency distribution for October 2017 compared to previous time periods. I have changed two columns to indicate the AUC mean BG and predicted HbA1c. AUC mean BG is the mean BG by calculating the area under the curve (AUC) of BG versus time. The predicted HbA1c uses the formula: AUC mean BG plus 88.55 divided 33.298. This formula is the least squares fit using my own personal mean BG versus measured HbA1c over many years. My particular HbA1c values are higher than many other individuals with the same mean BG. This is referred to as being a “high glycator.”
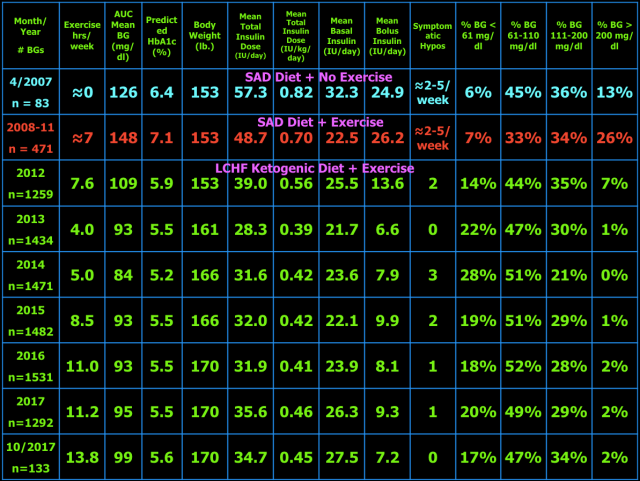
As presented in blog post #15 exogenous insulin cannot mimic normal insulin secretion, so persons with T1DM should not expect to have truly normal BG values at all times. They just need to be low enough to prevent long-term complications and not so low as to cause unpleasant hypoglycemic symptoms or less common but dangerous consequences including brain damage, seizure, injury, coma, or death. I have set my target BG range at 61-110 mg/dl because values in this range are not likely to lead to harm or complications of T1DM. Your target BG range should be determined with your physician because one size does not fit all. Normal BG is 96 ± 12 mg/dl (mean ± standard deviation (SD)) and coefficient of variation is 13% which is the weighted mean from these two studies (here and here) of continuous glucose monitoring in healthy subjects. The standard deviation and coefficient of variation are measures of BG variability which I believe are important in T1DM. However, be advised that clinical outcomes in T1DM (i.e. microvascular and macrovascular complications) have only been documented to correlate with measures of mean BG, particularly HbA1c. This does not mean that BG variability is not important, but it just has not been documented to correlate with outcomes and complications of T1DM. Achieving a normal standard deviation or coefficient of variation in T1DM would be difficult, if not impossible, with current exogenous insulin therapy (injected or pumped). Monitoring the standard deviation and/or coefficient of variation and finding ways to improve them to the best of one’s ability is desirable in my opinion. Following a low carbohydrate ketogenic diet is one such method of reducing BG variability, mean BG, insulin doses, and hypoglycemia. A ketogenic diet and MCT oil used on salads at dinnertime may also provide an alternate/additional brain fuel in the form of ketones to protect the brain when BG does go low. The alternative energy that ketones supply to the brain may prevent or blunt the sympathoadrenal response to hypoglycemia which in turn reduces or eliminates the symptoms of and harm from hypoglycemia. This hypothesis needs to be tested before it can be stated as fact. Having BG close to normal most of the time (some of which are hypoglycemic) also minimizes the symptoms of mild hypoglycemia and potentially the harm from hypoglycemia as well due to lack of activation of the sympathetic nervous system and adrenal gland responses to hypoglycemia i.e. sympathoadrenal-induced fatal cardiac arrhythmia, see here.
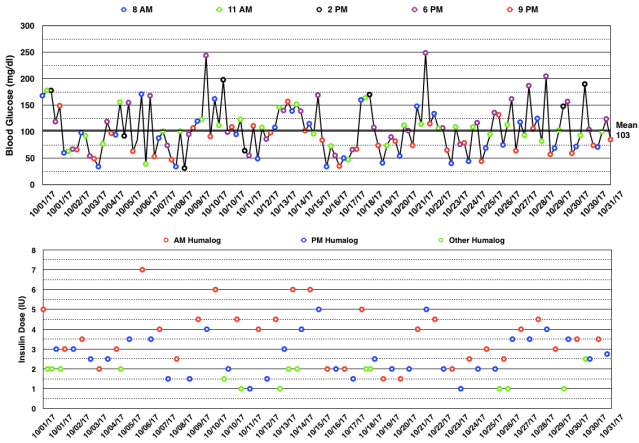
Below are my BG readings along with the Humalog (rapid-acting insulin) doses in October 2017. I adjust both the morning and evening meal-time doses based on the pre-meal BG reading and take extra correction Humalog doses (green circles) for high BG readings between meals. I returned to my previous pattern of high BG readings after weightlifting. This is primarily controlled by the basal insulin (Lantus) dose taken at dinnertime but that dose is determined by the fasting BG reading and thus cannot be adjusted to optimize all times of day. Those without diabetes can experience an increase in BG with intense exercise, see here. In those with T1DM the basal insulin dose may be enough to compensate for the increase in BG with intense exercise, but may also require a rapid-acting insulin dose to lower a high post-exercise BG.
The table below shows the BG variability results for current and previous time periods. The percentiles (10th, 25th, 75th, 90th) on the right show the spread of the BG readings about the median. The interquartile range, the difference between the 75th and 25th percentiles, is a measure of BG variability. In the middle of the table are the %Time in three BG ranges: %Time BG < 61 mg/dl (hypo) and the mean BG during that time, then %Time BG 61-110 mg/dl (target) and the mean BG during that time, and %Time BG > 110 mg/dl (hyper) and the mean BG during that time. The other measures of BG variability were defined and explained in blog post #10.

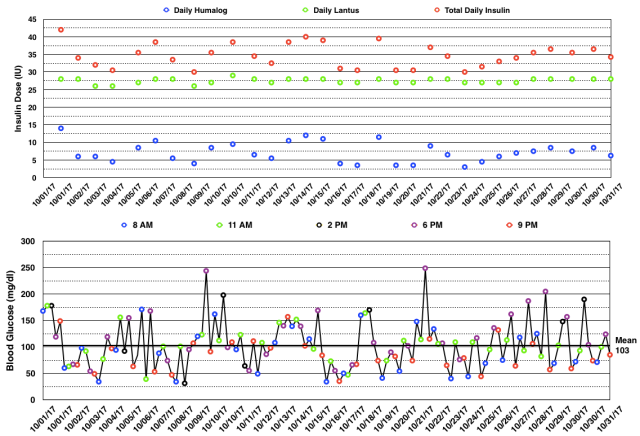
The daily insulin dose totals and BG readings are shown in the graphs below. You can see there was no consistent up or down trend in insulin doses and that the total daily insulin dose varied between 30 and 44 IU/day.
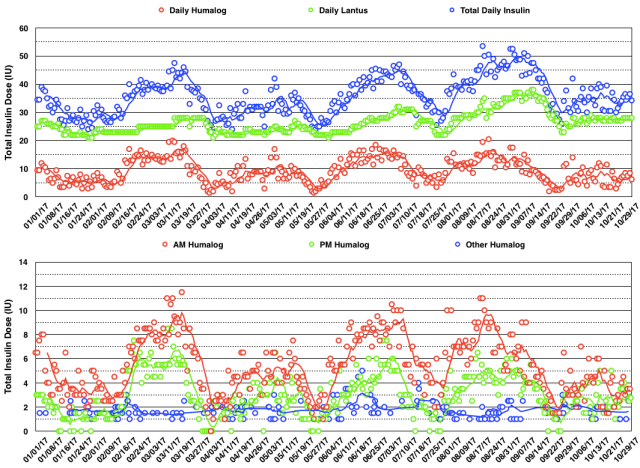
The daily insulin dose totals and the 7 day moving average for 2017 are shown in the graph below. You can see an oscillatory pattern with a period of about 8 weeks. In October there was some stabilization of insulin doses. I think it is too early to say that I have solved the problem of oscillating insulin doses, but I did change my procedure of drawing insulin from the vial into the syringe by not injecting air into the vial with a reused needle. It is possible that some old polymerized insulin could be reinjected into the vial which could cause inactivation of the insulin in the vial. This in turn would result in a progressive increase in insulin dose required until a new vial was used and then the doses would decline as a result of hypoglycemia from the more active insulin in the new vial. It’s a theory anyway.
In November, I will continue olympic weightlifting every day with three exercises per day one of which will be either snatch or clean and jerk once I am sure my shoulder has healed completely.
My Thoughts About Management of Type 1 Diabetes With A Ketogenic Diet
My goal of glycemic management in T1DM with a ketogenic diet is to keep BG as close to normal i.e. 96 ± 12 mg/dl (mean ± SD) as is safely possible (i.e. avoiding hypoglycemia) to avoid diabetic complications, a reduction in lifespan, and unpleasant symptoms of as well as injury and death from hypoglycemia. For me, a well-formulated whole-food nutrient-dense ketogenic diet, daily exercise, frequent BG measurements, and lower insulin-analog doses (Humalog/Lantus) have improved my glycemic control, hypoglycemic reactions, and quality of life. My current version of ketogenic diet has changed slightly since I last wrote about it in detail in blog post #9.
My current diet looks like this.
What I Cook & Eat
- Beef, grass-fed, including meat (85% lean), heart, liver, and kidney (liverwurst)
- Fish, mainly wild Alaskan salmon
- Canadian bacon (uncured pork loin)
- Lamb occasionally
- Chicken & Turkey occasionally
- Chicken Eggs
- Non-starchy vegetables (about 5% carbohydrate content by weight) including Cabbage (Red, Green, Napa), Kale, Collard Greens, Spinach, Bell Peppers, Leeks, Onions, Brussels sprouts, Home-made Sauerkraut from Red Cabbage, Bok-Choy, Broccoli, Cauliflower, Yellow Squash, Zucchini, Cucumber, Lettuce (Iceberg & Romaine), and some others.
- Fruit – Avocado, Tomatoes, Olives, Strawberries, Blueberries, Blackberries, lemon juice on fish and salads
- Root Vegetable: Raw Carrots
- Nuts & Seeds – Pepitas, Macadamia, Brazil, Pecan, Walnut, Pistachio, Cashew.
- MCT oil – a few tablespoons on salads
- Note: I developed an intolerance to milk prior to my diagnosis of T1D. I did try heavy whipping cream after starting my KLCHF diet, but am also intolerant of it. I do tolerate butter, but wanted to decrease my fat intake, so eliminated all dairy including cheese and yogurt.
What I Drink
Water (filtered by reverse osmosis), Unsweetened Tea & Coffee
What I Don’t Eat
- Grains – Wheat, Corn, Rice, Oats (there are many more) or anything made from them, which is too numerous to list here. Gluten is a protein present in a number of grains (all varieties of wheat including spelt, kamut, and triticale as well as barley and rye.) which can cause a number of medical problems for a significant portion of the population with gluten sensitivity or celiac disease. In my case, I avoid them due to their carbohydrate content.
- Starchy and most root vegetables – potatoes, sweet potatoes, yams
- Legumes – peas, beans, lentils, peanuts, soybeans
- High sugar fruits – includes most fruits except berries, see above.
- Sugar and the fifty other names used to disguise sugar.
- Vegetable Oils – Canola, Corn, Soybean, Peanut, Sunflower, Safflower, Cottonseed, Grape seed, Margarine & Butter substitutes, Shortening.
- All Processed Food-like Substances i.e., most of what is in the grocery store.
- I avoid restaurants except when traveling, and then order fish or steak with plain steamed non-starchy vegetables (no gravy or sauces that typically contain sugar, cornstarch, or flour) or salad.
- Refined, but healthy, fats – I have eliminated refined fats except MCT oil from my diet including butter, coconut & olive oils to improve body composition and remain in the 77kg olympic weightlifting weight class.
What I Don’t Drink
- Colas (both sweetened, artificially sweetened, and unsweetened).
- Fruit Juice except small amounts of lemon juice.
- Alcohol (can cause hyperglycemia or hypoglycemia in persons with diabetes).
- No artificial sweeteners, don’t need or like them.
When my entire diet is analyzed, 26% of my fat intake is from polyunsaturates (mainly from nuts and seeds), 56% is from monounsaturates, and 18% is from saturated fats. When my diet is broken down by macronutrients, I consume 170 grams of fat (or 68% of my total daily calories), 70 grams of carbohydrate, 30 grams of which is dietary fiber (or 12% of my total daily calories), and 110 grams of protein (or 20% of my total daily calories). In calories, it totals to 2,250 kcal/day.
My exercise regimen makes glycemic management more challenging, but I enjoy exercise and feel it has other health and lifespan-extending benefits. Hopefully, my BG values and variability as well as my lower insulin doses that result from my ketogenic diet and exercise are close enough to optimal to avoid any reduction in lifespan, diabetic complications, and harm from hypoglycemia, but only time will tell.

Curios if you use a CGM? Not to be critical, but i am somewhat perplexed by the volatility in both the glucose levels and the insulin doses reported, with a low carb diet. I have debated a keto diet myself, as a T1D for 18 years. Wanting data before making a decision, I was eager to see your results. I question how often you are actually in ketosis, versus? I would very much welcome a phone call if you have the time.
LikeLike
Hi Andrew. I have not used a CGM yet, but the FreeStyle Libre CGM was recently approved by the FDA here in the U.S. so I hope to give it a try soon.
Yes, my blood glucose (BG) and insulin doses are more volatile than I would like. I think my exercise contributes to that volatility but a lot of it is inherent to using exogenous insulin and having non-functioning beta cells. Do I think a low carb ketogenic diet contributes to the volatility? Definitely NOT. I have entered my data from prior to the ketogenic diet and the summary of that analysis is shown in the blog post that my BG levels were higher and the standard deviation was much higher. Many with T1DM are not even aware of how volatile their results are because they are not analyzing and graphing them the way you see in my blog. I would be interested in seeing your results analyzed and graphed in the same manner if you feel you can share them.
I am in ketosis by both blood and breath ketone measurements about 98% of the times that I have checked them. However the goal of using the ketogenic diet for T1DM is not to be in ketosis, rather ketosis is just a consequence of avoiding the dietary carbohydrates that leads to more hypoglycemia and hyperglycemia and requires additional insulin to process.
If you are satisfied with your BG results and you like your current diet, maybe a whole food low carbohydrate ketogenic diet is not necessary.
LikeLike
Thank you, Keith. I have read your book, and heard you podcast with Nourish Balance Thrive. I appreciate what you are doing and the manner in which you share your information. I don’t maintain written charts / graphs, but pay close attention to my Dexcom on a daily basis. I make lots of small adjustments during the day, typically not dosing more than 2 units of humalog at any time….but may do so 6+ times a day. My large meals are typically keto-like, meat and veggies. But I do eat carbs throughout the day in small amounts. My interest in keto is partly about BG control, but more so I am fascinated by the notion that an endurance athlete can perform for hours without carbs. I do a lot of cycling in the warmer months, 75 – 100 mile rides, and have often thought keto could be a good way to enhance this. As for the impact of weight lifting, yes I have experienced the impact this has on BG levels, and on leg day things can get interesting….. Curious if you use Creatine, and if you could share any thoughts on this. I have found it has a profound impact on BG, but have recently become interested if there are any studies on long-term use. I am starting to wonder if it has any impact on adrenal function / cortisol production.
LikeLike
In earlier blog posts I wrote about my experience with endurance training and doing triathlons. I took no carbs or food during an ironman distance triathlon due to having BG values between 150 and 250. However, BG values depend greatly on the basal insulin dose or pump rate at the time, so carbs may be necessary to bring up BG at times. I can’t comment on performance since I was not competitive in that sport. I switched to olympic weightlifting in Feb. 2015 while continuing endurance training mainly cycling and swimming since plantar fasciitis prevented me from running. About 4 months ago I stopped endurance training in the hopes that my weightlifting performance might improve to point I might be competitive at the Master’s level. Still waiting to see if that helped.
I started taking creatine on July 22, 2016, at 2.5 grams/day. I have taken it daily since. I picked that dose based on the amount of meat I eat and that it is made endogenously as well. I have not noticed any improvement or adverse effects from it. I researched it before buying it. This is a good review article, here. Creatine is inexpensive, makes sense for weightlifting, and at the dose I am taking is very unlikely to have any adverse effects. I have not noticed an effect on BG, but since I take the same amount at the same time of day every day, I might not notice a BG effect. If it adversely affects your BG and you are concerned about other side effects, it is probably best to stop using it as I doubt it has a huge impact on performance.
LikeLike
Keith,
Attached are my numbers for today, off Dexcom. This is a pretty typical day. The red line is 60 mg/dL, and the yellow is 130 mg/dL. It is rare that I go above 150 mg/dl. You can see on the left side that dinner got away from me last night (did not realize the amount of bread crumbs that were in a casserole), but with the CGM trend I was able to start correcting and take the peak off.
Sent from my iPad
>
LikeLike
Thanks Andrew, I guess attachments don’t attach to blog comments. Maybe try to paste a screenshot.
LikeLike